
The Complete Guide to CBCT Scanning in Dentistry: What Every Patient and Dentist Needs to Know
“You have been referred for a CBCT scan and have never heard of it. Or you are a dentist who orders them regularly but wants a deeper clinical reference. Either way, this guide is written for you — in plain, honest language that most medical content refuses to use.”
Why CBCT Changed Dental Diagnosis Forever
There is a moment every experienced dental radiologist remembers — the first time they showed a patient their own jaw in three dimensions. Not a flat shadow on a film. Not a grey, blurry panoramic image where roots overlap and anatomic structures superimpose on top of one-another. An actual 3D reconstruction: bone, teeth, nerve canals, sinuses — all dynamically viewable, all measurable without distortion, all unmistakably real.
That moment changes how patients understand their own treatment. And it changes what dentists can do.
Cone Beam Computed Tomography — CBCT — is now the gold standard for Dental Diagnostics in India and Worldwide. Yet despite being used in dental practices for over two decades, it continues to be an undervalued and minimally understood tool. Patients are anxious about radiation. Dentists sometimes underestimate what a specialist-reported CBCT can reveal. And a great deal of important clinical information gets lost when CBCT images are captured but never properly read.
This guide corrects all of that. Whether you are a patient who has been referred for a scan, or a dental professional wanting a comprehensive clinical inference — this is the most complete, accurate, and practically useful guide to CBCT in dentistry available today.
What Is a CBCT Scan? Understanding the Technology
CBCT stands for Cone Beam Computed Tomography. It is a specialised X-ray system that uses a cone-shaped beam of radiation to capture hundreds of images as the machine rotates around the patient’s head. Software then reconstructs these frames into a fully navigable three-dimensional dataset — a digital representation of the jaw, teeth, nerve canals, and sinuses that can be explored in any direction.
The key distinction is three-dimensional representation of anatomy. Every conventional dental X-ray — the OPG, the periapical, the bitewing — compresses a three-dimensional structure onto a flat plane. Depth, width, and precise positional relationships are lost in that compression. What sits behind what, how deep something extends, where exactly a nerve runs — none of this is visible on a 2D image. CBCT captures all of it accurately.
How the CBCT Machine Works
A CBCT scanner looks, to most patients, like a large half-ring or arch (gantry) that rotates around the head. The patient stands or sits — depending on the machine design — while the gantry, the rotating arm, completes one full or partial rotation. This takes approximately 8 to 40 seconds depending on the machine and the field of view selected.
During the rotation, an X-ray source and a flat-panel detector move in synchrony. The cone-shaped beam captures between 150 and 600 individual frames, each from a slightly different angle. Software then performs filtered back-projection — or iterative reconstruction in newer machines — to assemble these frames into a three-dimensional volume called the DICOM dataset. This dataset can be viewed as:
Axial slices — Cross-sections viewed from above, like looking straight down through the jaw
Coronal slices — Front-to-back cross-sections showing depth from front teeth to molars
Sagittal slices — Side-to-side cross-sections showing the jaw in profile
3D volume render — A full three-dimensional surface model of the jaw and teeth, rotatable in any direction
The specialist radiologists at DMD Imaging, always MDS-qualified Dental radiologists — review all of image sections systematically before writing the clinical report your dentist uses to plan treatment.
CBCT Was Designed Specifically for Dentistry
This is an important distinction that is frequently misunderstood. CBCT is not a medical CT scanner repurposed for dental use. It was engineered from the ground up for Dental and Maxillofacial imaging.
Medical CT scanners, used in hospitals for brain, chest and abdominal imaging, use a fan-shaped beam and are built to image large volumes with high soft tissue contrast. They are powerful but deliver a significantly higher radiation dose than dental imaging requires.
CBCT uses a smaller, cone-shaped beam focused precisely on the face and jaws. The field of view can be controlled from a small sectional volume of a few centimetres to a full skull volume. This precision dramatically reduces radiation dose compared to medical CT, while capturing far superior spatial detail for dental structures than any 2D dental X-ray and without any image magnification or distortion. It is, simply the right tool for the right anatomy.
CBCT vs OPG: What the Difference Actually Means for Your Diagnosis
The OPG — Orthopantomogram, also called a panoramic X-ray — is a very common full-mouth dental imaging investigation. It provides a single flat image of both jaws, all teeth, and the surrounding structures. For routine monitoring, initial screening, and general dental overview, it is a valuable, low-dose investigation that has been a cornerstone of dental diagnosis for over 60 years.
At DMD Imaging, every OPG is reviewed and interpreted by an MDS-qualified dental radiologist — because even a routine panoramic X-ray can contain findings that a non-specialist eye misses.
However, in many clinical situations, the OPG is fundamentally inadequate. This is not a criticism of the OPG as technology. It is a statement about the physics of two-dimensional imaging and its inherent limitations when applied to complex three-dimensional anatomy.
What an OPG Shows Well
An OPG provides reliable diagnostic information for overall dental overview, tooth development monitoring in children, gross pathology such as large cysts or extensive bone loss, general periodontal bone levels, and a baseline impression of the maxillary sinuses and jaw joints. For screening and routine monitoring, it remains appropriate and cost-effective.
What an OPG Cannot Show — and Why It Matters
The OPG’s fundamental limitation is projection. It collapses three-dimensional anatomy onto a flat image. In doing so, it cannot tell you:
Bone depth or width: The OPG shows bone height but not volume. Implant planning requires knowing how much bone exists in three dimensions — both height and bucco-lingual width. Without this, surgical planning is based on incomplete data.
Precise nerve canal position: The inferior alveolar nerve canal appears as a line on an OPG. Its exact three-dimensional position — depth, distance from the ridge, loops, bifurcations — cannot be assessed accurately without CBCT.
Root canal anatomy: Extra canals such as the MB2 in upper first molars, present in up to 96% of patients, are invisible on 2D imaging. Root curvature, calcifications, and resorption in the bucco-lingual plane are similarly hidden.
Sinus anatomy in detail: OPG shows the maxillary sinuses as overlapping shadows. CBCT shows membrane thickness, septae, floor topography, and any odontogenic connection in full three-dimensional detail.
Buccal and lingual bone: The outer and inner surfaces of the jawbone are completely invisible on OPG. Bone defects, dehiscences, and fenestrations on these surfaces — clinically important for implant planning and periodontal surgery — are hidden.
“A practical example: A patient referred for upper premolar implant planning. The OPG suggested 12 mm of bone above the apparent sinus floor. CBCT revealed actual available bone height of 4.5 mm at the proposed site — a sinus augmentation was required before any implant could be placed. This discrepancy is one of the most regularly encountered differences between OPG assessment and CBCT measurement in implant planning at DMD Imaging. ”
CBCT Radiation Safety: The Facts, Not the Fear
Radiation anxiety is one of the most common reasons patients delay or decline dental imaging. The concern is entirely understandable. But for dental X-rays, it is almost entirely unfounded — provided patients are given accurate numbers rather than generic reassurance.
Radiation Dose Comparison
The following table shows effective radiation doses for common dental and medical investigations, drawn from ICRP Publication 103 and NCRP Report 177:
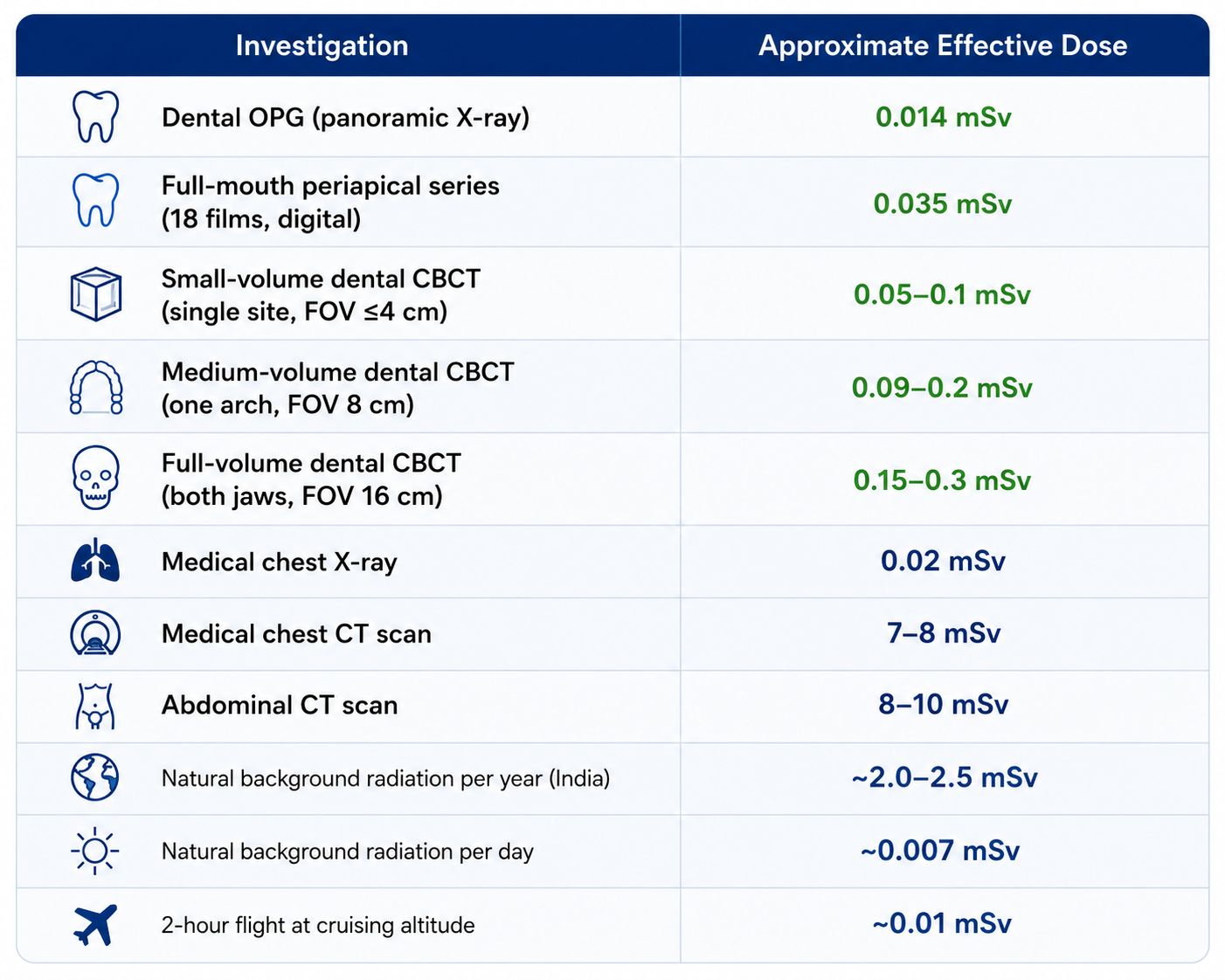
Source: ICRP Publication 103; NCRP Report 177; published dental dosimetry literature
To translate these numbers into plain language: a dental OPG delivers the same radiation as roughly two hours of natural background radiation — the radiation everyone receives every day simply from living on Earth. A small-volume dental CBCT, the most common type ordered for implant planning or endodontic cases, delivers the equivalent of one to two weeks of natural background radiation. Not years. Weeks. A full-volume CBCT is still 25 to 50 times less radiation than a standard abdominal CT scan.
The ALARA Principle at DMD Imaging
Every imaging protocol at DMD Imaging is governed by the ALARA principle — As Low As Reasonably Achievable. In practice, this means the field of view is selected to cover only the clinically relevant anatomy for each case. Machine parameters — kVp, mA, and exposure time — are optimised for each patient. Paediatric patients receive specific low-dose child protocols. Lead aprons are used for every patient. CBCT is recommended only when the clinical question cannot be answered by a lower-dose 2D investigation.
Pregnancy, Children, and Breastfeeding
Patients who are pregnant or suspect they may be pregnant should always inform the clinical team before any X-ray investigation. For dental CBCT with a lead apron, the radiation dose to the abdomen and foetus is negligible — less than 0.001 mSv. For non-urgent cases, deferring until after the first trimester is standard practice. The decision is made on a case-by-case basis by the radiologist and referring clinician.
For paediatric patients, modern CBCT units have child-specific low-dose protocols and smaller field-of-view options that significantly reduce exposure below adult scan parameters. CBCT in children is reserved for specific clinical indications — impacted canines, jaw assessment, surgical planning — not routine monitoring.
Breastfeeding patients can be reassured fully: CBCT radiation does not affect breast milk. No change to breastfeeding is required before, during, or after the scan.
Clinical Uses of CBCT: When 3D Imaging Changes Treatment
The question dentists most appropriately ask is not “what does CBCT show?” but “when does it change what I do?” This is the right question — because a scan that does not change clinical decision-making does not justify its dose or cost. The evidence base across multiple specialties is consistent: in appropriately selected cases, CBCT significantly changes diagnosis and treatment planning in 30 to 60 percent of cases compared to 2D imaging alone.
Implant Planning and Oral Surgery
Implant placement is the single most common reason CBCT is requested in dental practice, and the area with the strongest evidence base for its clinical necessity. Safe implant placement requires knowing, to sub-millimeter precision:
Bone height: The vertical distance from the alveolar crest to the nearest anatomical boundary — the inferior alveolar nerve canal below, or the sinus floor above. This determines the maximum safe implant length.
Bone width: The bucco-lingual width of the ridge at the proposed site. This determines whether a standard-diameter implant is feasible or whether bone grafting is required and dictates the correct implant axis.
Bone density: Classified from D1 (very dense cortical bone) to D4 types (soft, poorly mineralised cancellous bone). Density influences implant design, primary stability expectations, and healing protocol.
Inferior alveolar nerve canal position: The IAN canal runs through the body of the mandible. Damage to it causes transient or long-lasting loss of sensation in the lower lip and chin. The standard surgical safety margin is 2mm from the implant apex to the canal — this measurement requires CBCT.
Sinus floor anatomy: The maxillary sinus floor is not flat. It contains recesses, septae, and significant individual variation. Only CBCT maps this anatomy accurately enough for safe upper posterior implant planning.
For wisdom tooth surgery, CBCT is particularly valuable when OPG suggests proximity of the lower third molar roots to the inferior alveolar nerve. CBCT clarifies whether this relationship is genuinely intimate or the result of 2D projection overlap — a distinction that changes the surgical approach and the risk counselling entirely.
Endodontics: Root Canal Treatment and Retreatment
Root canal treatment fails most commonly not because of inadequate technique, but because of undetected anatomy. CBCT addresses this directly.
The MB2 canal in the mesio-buccal root of the upper first molar is present in 56 to 96 percent of patients, depending on the population studied. It is frequently invisible on periapical X-rays taken at standard angulations because of root overlap and palatal root superimposition. On CBCT, it is almost always identifiable. Its presence — and its absence in a previously treated tooth — is one of the strongest predictors of endodontic success or failure.
Root resorption — both internal (the tooth dissolving from the inside) and external (destruction from the root surface outward) — is frequently invisible on 2D imaging until advanced. CBCT detects resorption earlier, characterizes its exact extent and location, and guides the treatment decision between conservative endodontic management, surgical intervention, and extraction.
Periapical pathology is another key area: a dark shadow on a periapical film becomes a characterized lesion on CBCT — defined by its three-dimensional extent, cortical plate involvement, and morphology. The distinction between a periapical granuloma and a radicular cyst changes whether endodontic treatment alone will suffice or surgical enucleation is required.
Orthodontics, Airway and Facial Growth, TMJ Evaluation
CBCT has transformed orthodontic diagnosis in three specific clinical areas. Impacted canine localisation — determining whether an upper canine is on the palatal or buccal side of the arch — fundamentally changes the surgical approach, the orthodontic mechanics, and the prognosis. This determination cannot be reliably made from 2D imaging. CBCT provides the definitive answer.
The oropharyngeal airway space has become an important predictor of many problems in the dento-facial region including Sleep apnea. Full FOV CBCT study and AI-driven software tools now enable assessment of the oropharyngeal airway volume and help narrow down or manage potential causes for sleep disorders in the dento-facial region.
For patients with significant jaw discrepancy considering orthognathic surgery, CBCT-derived lateral cephalograms and 3D measurements provide more accurate anatomical data than conventional 2D cephalometry. They also enable virtual surgical planning with realistic soft tissue prediction, quantification of facial asymmetry or discrepancies in the upper and lower alveolar arches.
CBCT is considered as the Gold standard for hard-tissue (bone) evaluation of the Tempromandibular Joints, and enables characterization of degenerative joint disease or arthropathy even at an early or initian stage. At DMD Imaging, our team has developed a novel protocol for Closed & Open-mouth TMJ CBCT study, where we are able to provide accurate assessments of the bony structures, joint translation and provide predictive assessment of TMJ Disc derangement for patients with joint pain and clicking.
Upper incisor root resorption caused by impacted canines is a clinical concern requiring 3D quantification. CBCT allows measurement of resorption volume and surface area, guiding the urgency of canine exposure and the prognosis for the affected incisors.
Periodontics: Bone Defect Assessment and Surgical Planning
2D periapical and bitewing X-rays show interproximal bone levels but cannot characterise buccal and lingual bone — those surfaces are completely invisible on flat-panel imaging. CBCT provides three-dimensional defect morphology: whether a bone defect is a one-wall, two-wall, three-wall, or circumferential defect determines regenerative potential and the appropriate treatment approach.
Furcation involvement, particularly in upper molars where buccal, mesial, distal, and palatal furcation areas must each be assessed individually, is far more accurately characterised on CBCT than on 2D film. Endo-perio lesion differentiation — distinguishing a primary endodontic lesion from a primary periodontal lesion from a true combined lesion — changes the treatment plan entirely. CBCT routinely resolves this diagnostic ambiguity.
Jaw Pathology, Cysts, and Incidental Findings
Jaw cysts, benign tumours, and oral pathology visible on CBCT include radicular cysts, dentigerous cysts, odontogenic keratocysts (which tend to grow along the jaw without expanding the cortex), and ameloblastomas, which show characteristic cortical expansion and internal bony septations. CBCT defines the extent of each lesion, its cortical plate involvement, and its relationship to adjacent teeth and nerves — information essential for surgical planning and margin definition.
Beyond the primary referral question, CBCT frequently reveals findings that change patient outcomes beyond dentistry. At DMD Imaging, our radiologists have identified calcified lymph nodes, carotid artery calcifications, cervical spine anomalies, and maxillary sinus pathology as incidental findings in CBCTs taken for entirely unrelated dental purposes. These findings, flagged in our reports, have in several documented cases led to medical referrals that identified conditions the patient did not know they had.
What to Expect During Your CBCT Scan: A Complete Patient Guide
Before the Scan: Preparation
There is no special preparation required for a dental CBCT. Unlike many medical investigations, you do not need to fast, adjust medication, or arrange transport. What you should do:
Remove all metal before your appointment: Earrings, necklaces, hair clips, facial piercings, hearing aids, and removable dental prostheses must be taken off before scanning. Metal objects cause streak artefacts — bright white lines that radiate from the metal and can obscure adjacent anatomy. If you have fixed orthodontic appliances such as braces, inform the radiographer, as these may affect image quality in certain areas.
Bring your referral letter: The referral tells the radiologist exactly what clinical question the scan needs to answer, enabling the correct field of view and protocol to be selected. It ensures the report addresses your specific situation rather than providing only a generic structural description.
Wear comfortable clothing with a low neckline: The machine needs unobstructed access to your neck and jaw area.
Inform the team if you are pregnant or may be pregnant.
During the Scan
Most patients are surprised by how quick and simple a CBCT appointment is. Here is what happens:
Positioning: The radiographer will position you in the machine using adjustable chin and head supports to stabilise your head during the rotation.
Bite block: You may be asked to bite gently on a small plastic peg to separate the upper and lower teeth slightly, helping the software distinguish adjacent tooth surfaces.
Lead apron: A lead apron will be placed around your shoulders.
The scan: The radiographer steps behind a protective screen — standard radiation protection practice, since they perform multiple scans daily while you have one — and starts the machine. The gantry rotates smoothly around your head. Nothing touches your face. There is no injection, no contrast medium, no discomfort.
Stay still: The most important thing you can do is remain completely still for the 20 to 40 seconds of scan time. Even swallowing causes motion artefact that blurs the image and reduces diagnostic quality.
After the rotation, you can eat, drink, drive, and continue your day immediately. There is no recovery period of any kind.
After the Scan: Your Report
After the scan, the DICOM dataset is sent to the reporting radiologist. At DMD Imaging, this is always an MDS-qualified dental radiologist — not a radiographic technician, not a general medical radiologist, and not an automated AI system.
Report turnaround at DMD Imaging: OPG and simple 2D investigations are typically reported same day, within 2 to 4 hours. CBCT and complex 3D investigations are reported same day to 24 hours.
You receive a notification with a secure link to your digital report, accessible in a browser-based viewer without any software installation. Your report includes a plain-language patient summary explaining the main findings in terms a patient can understand, the full clinical radiology report in technical language for your dentist, and DICOM files that your dentist can open in any treatment planning software.
If any term in your report is unclear, you have every right to ask your dentist — or to call our radiologist team directly. That direct accessibility is a commitment DMD Imaging has maintained since 2011.
How to Read Your CBCT Report: A Plain-English Glossary
CBCT reports are written in clinical language for the treating dentist. But patients deserve to understand what their own report says. Here are the most common terms you may encounter:
Periapical radiolucency: A dark area at the tip of a tooth root. This indicates bone destruction at the root apex, usually caused by infection from a non-vital (dead) tooth. It may be completely asymptomatic. It requires treatment.
Furcation involvement: Bone loss at the point where the roots of a back tooth divide. It indicates advanced gum disease in that area. Severity is graded from I to III depending on how much bone has been lost between the roots.
Inferior alveolar canal: The bony channel running through the lower jaw containing the nerve and blood vessels. Its position is critical for implant surgery and wisdom tooth removal.
Maxillary sinus: The air-filled space behind your cheekbones, above your upper back teeth. Upper molar and premolar roots often sit close to or within the sinus floor. Dental infections can cause secondary sinus disease.
Mucosal thickening: Swelling or thickening of the sinus lining. Can be a sign of sinus infection or inflammation, sometimes of dental origin (odontogenic sinusitis).
Cortical plate: The hard outer wall of the jawbone. “Intact” means the bone boundary is preserved. “Thinned,” “expanded,” or “perforated” suggests a lesion is affecting the outer jaw wall.
Radiolucent lesion: A dark area in the bone where normal bone has been replaced by tissue — fluid, infected material, or soft tissue. Includes cysts, abscesses, and some tumours.
Radiopaque or calcification: A bright white area indicating calcium deposits. Can be benign or clinically significant depending on location and morphology.
Field of view (FOV): The volume of tissue that was imaged — small (up to 4 cm), medium (8 to 10 cm), or large (12 cm or more). Determines which structures are visible and influences the dose received.
CBCT Scan Cost in India: What You Should Know
CBCT scan pricing in India varies significantly depending on the type of centre, field of view selected, equipment quality, and — most importantly — whether a specialist radiologist review and written report are included.
Typical Price Ranges in Delhi NCR 2026
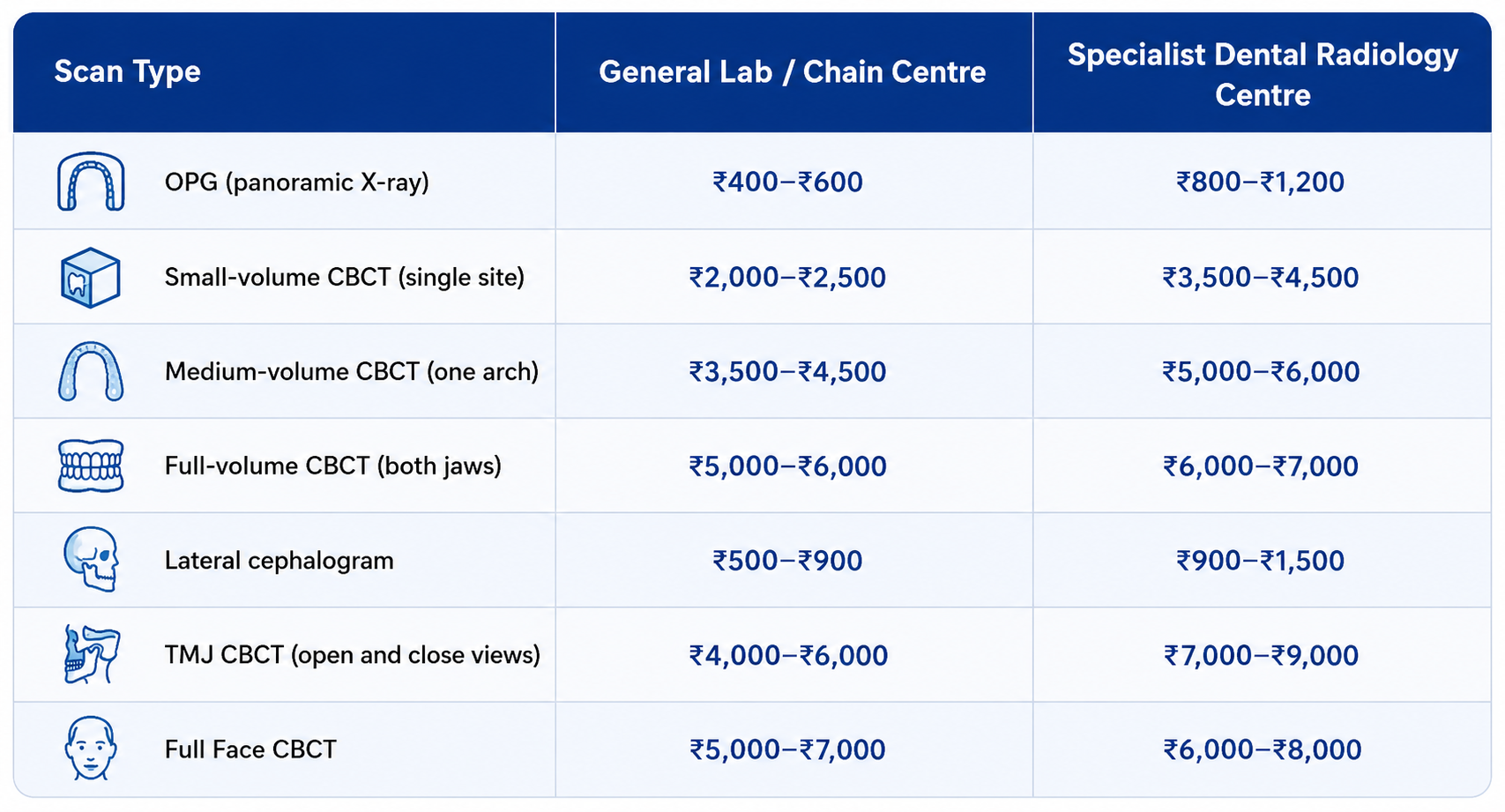
Note: Prices are indicative for Delhi NCR and vary by location. Confirm current pricing directly with the centre.
Why the Price Difference Exists — and Why It Matters
The price gap between a general diagnostic lab and a specialist dental radiology centre is not arbitrary. It reflects three concrete differences:
Equipment quality: CBCT machines vary enormously in resolution, dose efficiency, and software capability. A 75-90 micron resolution Full/ Large CBCT, as operated at DMD Imaging, provides significantly more diagnostic detail than a 200-micron medium FOV machine — particularly for small structures such as extra root canals, fine bony trabeculation, and early cortical changes.
Reporting quality: The most significant value-add in specialist dental radiology is the report. An OPG processed and printed at a general lab costs ₹400. An OPG reviewed by an MDS-qualified dental radiologist with a structured written clinical report addressing the specific referral question costs more. The additional cost buys findings that generic processing misses.
Radiologist versus technician review: Not all centres describing themselves as dental imaging centres employ qualified dental radiologists. If the person reviewing your CBCT is a radiographic technician, a general radiologist, or an automated system rather than an MDS-trained dental radiologist, the clinical value of the report is substantially reduced. The scan may look the same. The interpretation is not.
For any investigation that will guide a surgical decision — implant placement, wisdom tooth removal, jaw surgery, complex root canal treatment — the difference between a well-reported specialist CBCT and a processed scan from a general lab is the difference between a safe surgical plan and a plan based on incomplete information. The cost difference is measured in hundreds of rupees. The consequence of a missed anatomical finding in an implant case is not.
The Right Imaging, Reported by the Right Specialist
CBCT has not replaced clinical examination, periapical X-rays, or the panoramic radiograph (OPG). What it has done is fill the diagnostic gap that two-dimensional imaging leaves in cases where three-dimensional information is clinically essential.
The evidence is clear: in implant planning, endodontics, dento-facial orthodontics, Airway & TMJ assessment, periodontal surgery planning, and jaw pathology assessment, CBCT changes clinical decisions in a significant proportion of cases compared to 2D imaging alone. It reduces surgical complications. It catches findings that would otherwise be missed. And when reviewed by a specialist dental radiologist, it provides a clinical intelligence layer that fundamentally changes the quality of the treatment plan.
For patients: if you have been referred for a CBCT, you have been referred because your dentist needs information that only three-dimensional imaging can provide. The scan is safe, quick, and painless. The report you receive will be the most detailed picture of your jaw anatomy that has ever existed.
For dentists: the value of a CBCT is not the machine that takes it. It is the specialist who reads it. If your current imaging partner is delivering processed scans without specialist radiological reporting, clinical decisions are being made on incomplete information.
“At DMD Imaging, we have built 15 years of specialist dental radiology practice — from India’s first dedicated dental CBCT centre in 2011 to five centres across Delhi NCR today — on one principle: every scan deserves a specialist’s eyes. If you have questions about your CBCT report or the right investigation for your clinical situation, our radiologist team is reachable directly. That is what we are here for.”
Frequently Asked Questions About CBCT
-
No. A CBCT scan involves no injections, no physical contact with the machine, and no discomfort of any kind. The gantry rotates around you while you remain still. The only thing you may notice is the sound of the machine moving.
-
The scan rotation itself takes between 8 and 40 seconds. Your total appointment time, including registration, positioning, the scan, and checkout, is typically 20 to 30 minutes.
-
At most specialist dental radiology centres in India, including DMD Imaging, a referral from a dentist or oral surgeon is required or strongly recommended. The referral ensures the correct field of view is selected and that the report is written in the context of your treatment plan.
-
There is no fixed maximum. The decision is made based on clinical need, following the ALARA principle. If a new clinical question arises — a new treatment site, a change in clinical presentation, or a post-surgical assessment — a repeat scan is clinically justifiable. Your radiologist can advise on appropriate imaging intervals for your specific situation.
-
Always inform the clinical team if you are pregnant or may be pregnant before any X-ray investigation. The radiation dose to the abdomen from a dental CBCT with a lead apron is negligible — less than 0.001 mSv. For non-urgent cases, deferring until after the first trimester is standard practice.
-
Yes. CBCT radiation does not affect breast milk. No change to breastfeeding is required before, during, or after a dental X-ray investigation.
-
Both use X-ray tomography to create cross-sectional images. CBCT uses a cone-shaped beam designed for the head and jaw, delivers a fraction of the radiation dose of medical CT, and provides excellent bone and dental detail with limited soft tissue contrast. Medical CT delivers higher radiation, provides better soft tissue contrast across larger body volumes, and is generally not appropriate for routine dental investigations.
-
CBCT is a bone imaging tool. It is excellent at showing bone destruction and cortical changes that may accompany oral malignancy. However, CBCT does not show soft tissue tumours with the clarity required for cancer diagnosis — that requires MRI. Definitive cancer diagnosis always requires biopsy and histopathology. CBCT may be part of the diagnostic workup but is not a screening tool for oral cancer.
-
At DMD Imaging, every scan — including every OPG — is reviewed and reported by an MDS-qualified dental radiologist. This is not universal practice. When booking dental imaging anywhere, ask specifically who will review and report your scan. That answer will tell you a great deal about the quality of the service.
-
A dark area at the tip of a tooth root, indicating that bone is being destroyed at the root apex — usually by infection from a non-vital tooth. It may be completely painless. It requires treatment to prevent spread.